Eyelid Correction: Almost Always Much More Than Just “Removing Droopy Lids”
The eyes play a major role in human expression — they are the mirror of the soul. In this context, the eyelids and their surrounding areas are of great importance. Many people suffer from droopy eyelids, eye bags, dark circles, or sagging lateral eyebrows and feel less attractive as a result (“Doctor, people keep asking me why I look so tired…”). We can offer correction of all these problem areas and help you feel comfortable and confident in your appearance again.
Eyelid Lift: Beautiful Eyes Are Not a Question of Age
Over the course of life, changes in the skin lead to drooping eyelids and sagging eyebrows. Although this is a completely natural part of aging, it undeniably affects one’s appearance. Our eyelids and their surrounding areas (brows, midface) have a strong influence on whether we appear sad, happy, tired, or refreshed. They frame our eyes and play a decisive role in our facial expression. As a result, eye bags (fat bulges beneath the eyes), droopy eyelids (sagging upper lids), or wrinkled lower eyelids make us look tired and older.
Correction of the eyelids and their surrounding areas is among the most demanding procedures in aesthetic plastic surgery — and, unfortunately, often underestimated. To help you better understand the complexity of aesthetic eyelid surgery and the related issues, we will first outline the individual problem areas, then describe the surgical techniques used for their correction, and finally present possible combination procedures.
Anyone considering surgery should first clearly identify what specifically bothers them about their eyelids or surrounding areas and what they wish to correct. Together with the consulting physician, an evaluation will then be made to determine what can be done, and a personalized treatment plan will be developed.

The following aspects should be considered when analyzing the eyes:
- Position of the eyebrows
- Upper eyelids
- Lower eyelids
- Position of the outer eye corner compared to the inner corner (canthal tilt)
- Eye bags
- Dark circles
- Festoons
Example and analysis of a typical appearance of the eyes of a 52-year-old female patient
- Drooping upper eyelids (dermatochalasis), with pronounced excess skin on the sides mainly because the lateral eyebrows have descended significantly — not because there is actually more skin excess in that area.
- Laterally drooping eyebrows
- Excess skin on the lower eyelids
- Eye bags
- Dark circles under the eyes
- Negative canthal tilt (the outer eye corner is positioned slightly lower than the inner one — giving a “sad” or “hound-dog” look)
Note: Festoons (see below) are not present.

Treatment concept:
- Upper eyelid lift
- Elevation of the lateral eyebrows
- Lower eyelid tightening + canthopexy
- Correction of eye bags by downward fat repositioning
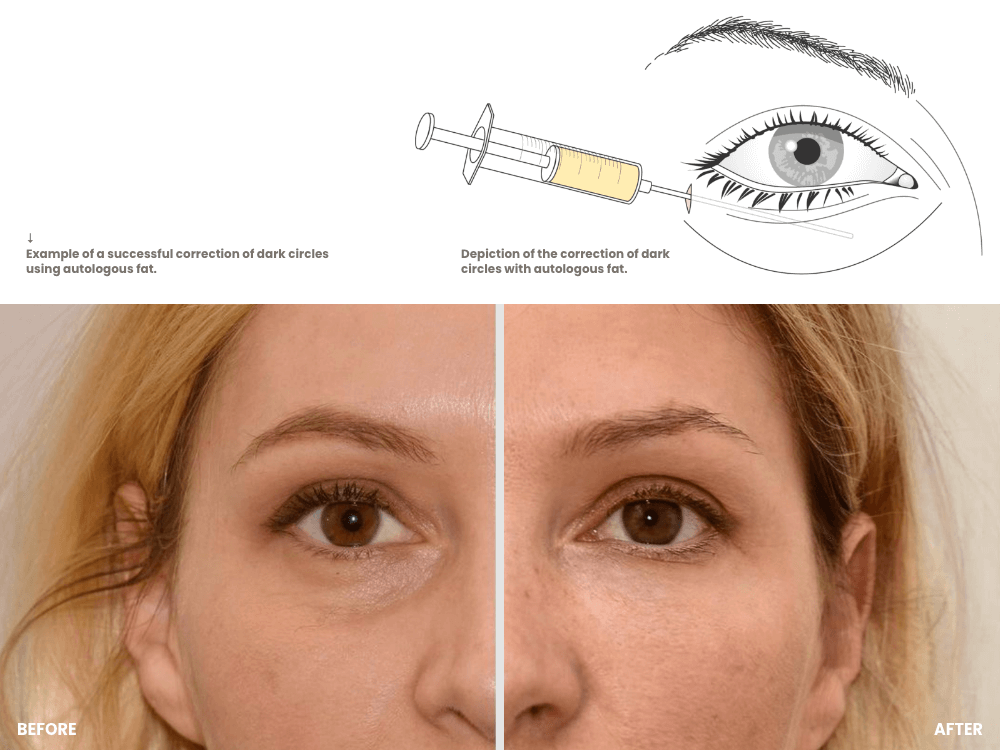
- Correction of dark circles by upward fat repositioning combined with supplementary autologous fat transfer
These procedures are possible as part of eyelid correction surgery
- Upper eyelid lift (correction of droopy eyelids)
- Elevation of the outer eyebrows (pseudo-droopy eyelids) without forehead lift
- Elevation of the outer eyebrows combined with upper eyelid lift (most common procedure)
- Elevation of the inner eyebrows without forehead lift
- Injection of autologous fat into the upper eyelid crease to correct hollow eyes
- Correction of eye bags (either by removal or by fat repositioning, depending on severity and the simultaneous presence of dark circles)
- Correction of dark circles by autologous fat transfer alone
- Surgical correction of dark circles through fat repositioning, possibly combined with autologous fat transfer
- Lower eyelid tightening — a demanding procedure as additional measures are required to prevent ectropion
- Correction of negative canthal tilt (“hound eyes” → “cat eyes”)
- Correction of festoons (alone or in combination with lower eyelid tightening — by far the most challenging procedure in aesthetic eye surgery, as several additional measures are needed to prevent ectropion)
- Brow lift (= forehead lift) when no actual skin excess is present and the descended forehead skin is primarily responsible for the tired appearance or the (apparent) excess skin
- Eyelid correction with laser
Causes and symptoms of drooping eyelids (hooded eyelids)
The natural proteins elastin and collagen, which occur in human skin, are responsible for a firm and even skin appearance. Over time, the skin gradually loses these proteins, resulting in a loss of elasticity and the formation of wrinkles (hooded eyelids). The often accompanying (sad) emotional or tired expression is, of course, undesirable.
Hooded eyelids do not only occur in older individuals but are quite often seen in younger people as well (sometimes as early as age 18–20), along with dark circles and eye bags. In these cases, the cause is typically genetic predisposition — this is neither pathological nor dangerous. Hooded eyelids (as well as dark circles and eye bags) can, of course, be surgically corrected even at a young age, provided that the indication is appropriate and the expectations are realistic.
- The development of sagging eyelids is promoted by the following factors:
- Unhealthy diet
- Smoking
- Lack of sleep
- Sun exposure
- Alcohol consumption
- Stress
Upper eyelid lift is performed almost exclusively for aesthetic reasons.
Hooded eyelids (medical term: blepharochalasis) occur equally in both women and men, almost always on both sides and only rarely on one side. In most cases, eyelid surgery (medical term: blepharoplasty) is performed for aesthetic reasons. However, in severe cases it can also lead to visual impairment (medical term: visual field restriction), in which case the operation is covered by public health insurance if performed in a public hospital.
Every patient can, of course, decide for themselves at what age they wish to undergo an eyelid lift; it mainly depends on how pronounced the excess skin is and how much it bothers them. During surgery, the excess skin on the upper eyelid is removed. A smooth, symmetrical, and natural result is achieved by carefully measuring and marking the exact amount of excess skin on the eyelid before the procedure. Removing the redundant skin tightens the eyelids. In some cases, a small amount of fat tissue in the upper eyelid area also needs to be removed.
There are, of course, limits to eyelid tightening, and knowing exactly how much correction is ideal to combine rejuvenation with naturalness can only be gained through many years of surgical experience and a large number of procedures. My advice: during your initial consultation, make sure to ask for plenty of before-and-after photos, evaluate the naturalness of the results, and have the surgical concept clearly explained and justified.
The incision must naturally be placed in such a way that the scars remain as inconspicuous as possible. This is almost always achievable for the upper eyelids if the incision is made along the upper eyelid crease (usually at 7–8 mm) and, for the lower eyelids, sharply along the lash line. If the procedure is successful, the eyes appear more radiant, the gaze becomes more open, and the scars soon become barely visible.
Causes and symptoms of drooping eyebrows – completely or only laterally
The skin of the face, the eyelids, and naturally also the forehead skin are subject to the same aging process. In the face, the skin sags and becomes wrinkled; on the eyelids, excess skin and wrinkles develop. In the forehead area, the eyebrows begin to descend because the connective tissue bands in the forehead also loosen. However, it has been shown that the eyebrows almost never descend symmetrically but rather predominantly on the sides at first (75–85%). This often results in the eyebrows being slightly lowered only on the sides, creating the appearance of excess skin on the upper eyelids (pseudo-hooded eyelids). In such cases, it is sufficient to lift the eyebrows laterally, and the symmetrical and open upper eyelid crease is restored through this maneuver alone.
Methods of eyebrow lifting – lateral or full
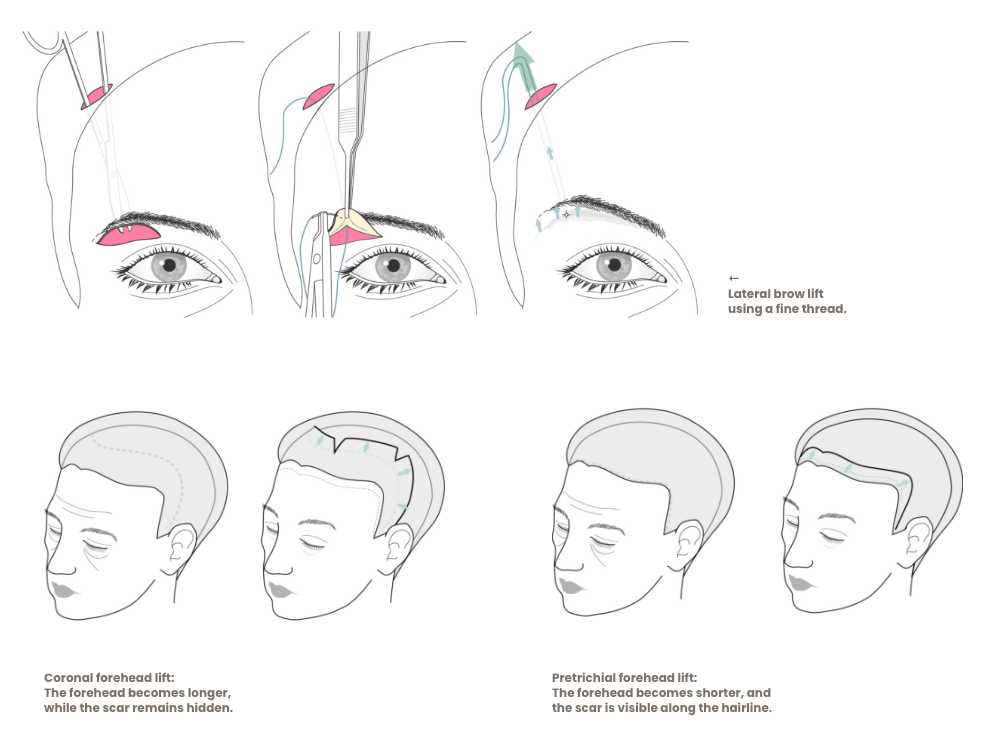
There are essentially three methods to lift the eyebrows laterally:
- By removing a crescent-shaped strip of skin above the eyebrow (leaves scars and is not effective, therefore I never perform this method)
- By anchoring the lateral eyebrow to the bone (periosteum) of the outer eye socket; this method is effective, but I prefer the thread technique (next point) because it allows the brows to remain more mobile (facial expression!)
- By lifting the lateral brow with a thin thread anchored in the temple area at the chewing muscle (in my view, the method of choice – performed more than 800 times)
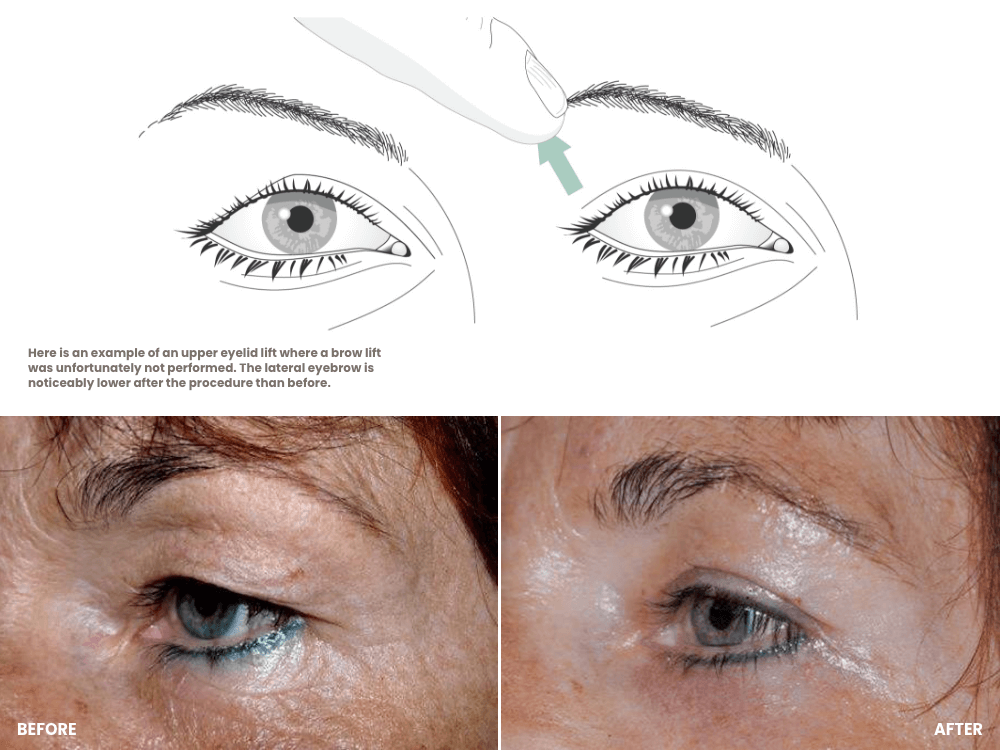
If there is also excess skin on the upper eyelids, particularly more pronounced laterally than in the middle, the combination of upper eyelid lift and lateral brow lift is the treatment of choice. Naturally, less skin needs to be removed from the upper eyelid when the lateral brows are lifted at the same time. This combination procedure is used in almost 80% of my patients undergoing upper eyelid tightening, confirming the fact that in most people, the lateral forehead skin sags earlier and more strongly than the central part.
If, however, the eyebrow has descended across its entire width, resulting in a “stern” or “frowning” appearance, a complete eyebrow lift should be considered.
There are essentially two methods to lift the eyebrows completely:
- Forehead lift (brow lift): This procedure is highly effective, although rather uncommon in our regions; the results, however, are truly impressive and can even be life-changing. The incision is made either along the hairline (for a high forehead) or within the hair (for a low forehead — the so-called “coronal” incision), and the forehead skin is tightened upward. It is therefore a more extensive or invasive procedure.
- Brow lift using threads, as with the lateral lift, but the anchoring is done in the center of the forehead at the bone. This approach is simple and minimally invasive but naturally less effective. However, if the lift required is no more than 8–10 mm, this method is quite suitable.
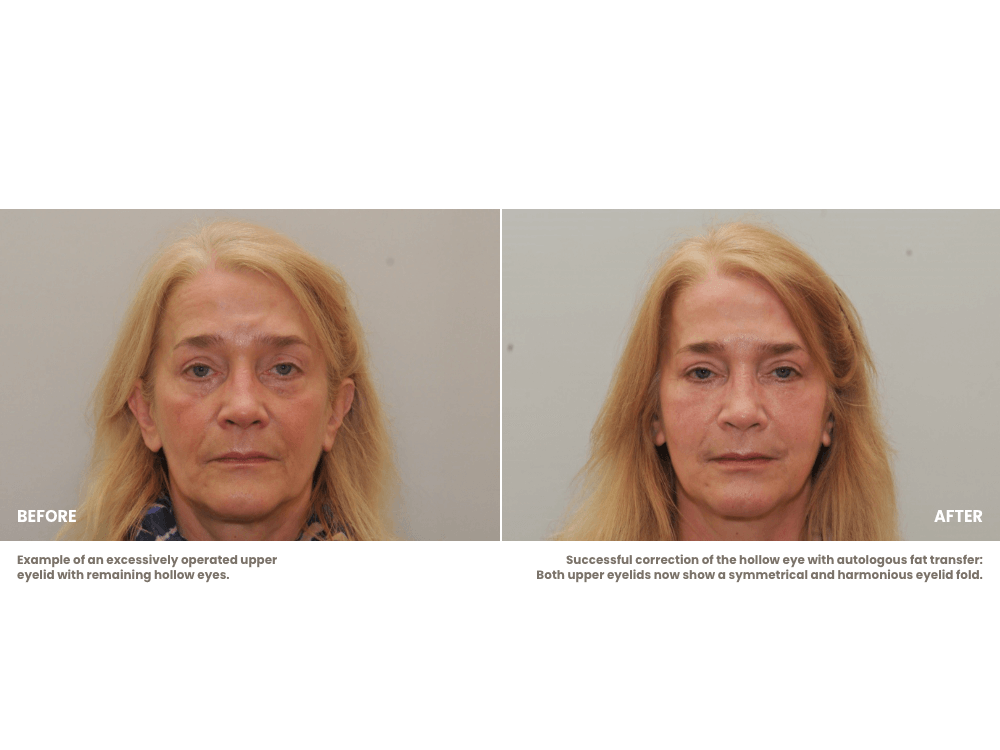
Hollow upper eyelids (sunken upper eyelids)
Many people have a very wide upper eyelid crease, where the eyeballs appear relatively prominent. From the front, one can see comparatively deep into the eye sockets. This is often perceived as unattractive and bothers many individuals. Correcting this condition is an essential part of the spectrum of eyelid surgery.
Under no circumstances should additional skin be removed in this situation, as that would further accentuate the hollow-eyed appearance. On the contrary, volume must be added, which pushes the upper eyelids forward and narrows the eyelid crease. The treatment of choice for hollow eyes is therefore autologous fat transfer. We always enrich the fat with PRP (platelet-rich plasma) to make it smoother and easier to model, while also improving its survival rate.
Solution: Autologous fat transfer
Causes and appearances of eye bags
Some people might assume that eye bags are caused by tears — but that is not the case. Eye bags have nothing to do with tears. They are located below the eyelids, beside the nose, and appear as bulging, cushion-like swellings. Eye bags always lie above any dark circles that may occur simultaneously. They consist of fat pads that normally sit beneath the eyeball but, due to connective tissue weakness, slip forward. The severity can vary greatly, and they may even appear at a very young age — during the teenage years or early adulthood. In younger individuals, eye bags are naturally not combined with dark circles, but from the age of about 35–40, they almost always are.
Misdiagnosis: Impaired lymphatic drainage / swelling
Some people complain of fluctuating swelling under the eyes, which is often most pronounced in the morning and subsides throughout the day. This is usually due to metabolic fluid accumulation in the connective tissue and fat of this area, or sometimes a lymphatic drainage disorder. Even sleeping face-down on the pillow can cause noticeable morning swelling in the midface. Fluid accumulates under the eyes because it cannot drain properly. If the swelling disappears during the day, these are not true eye bags. In such cases, the cause is often diet-related (e.g., alcohol consumption or allergens) or due to sleeping habits, which should be adjusted accordingly.
How are eye bags corrected?
1) Eye bags without dark circles (in younger individuals)
When eye bags appear at a very young age, treatment involves either removing the protruding fat or pushing it back into place while tightening (reinforcing) the connective tissue fascia that normally holds the fat beneath the eye. This procedure is performed on the inside of the lower eyelid (medically: transconjunctival), and therefore leaves no visible scar.
However, it often turns out that this procedure alone does not achieve an optimal result. It is difficult to remove just the right amount of fat or reposition it precisely enough to make the lower eyelid area both smooth and naturally full. For this reason, I regularly combine this procedure with autologous fat transfer, in which the lower eyelid area is gently filled using very fine cannulas to eliminate irregularities, leaving the region full, smooth, and without dimples. We always enrich the fat with PRP (platelet-rich plasma) to make it soft and moldable and to increase the survival rate of the transplanted fat.
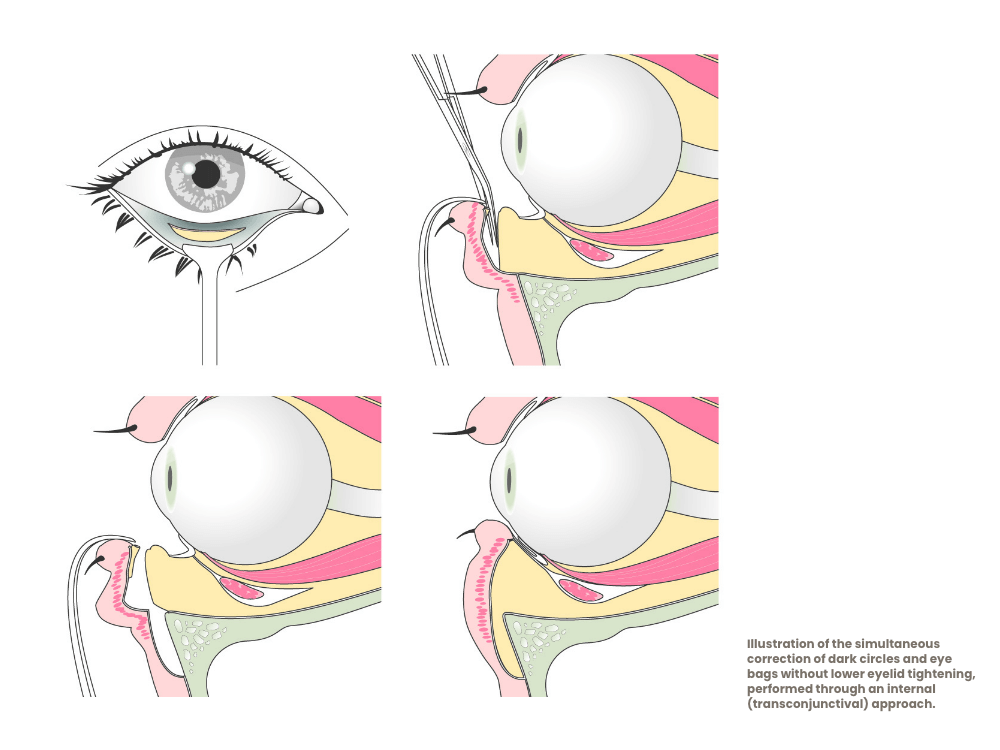
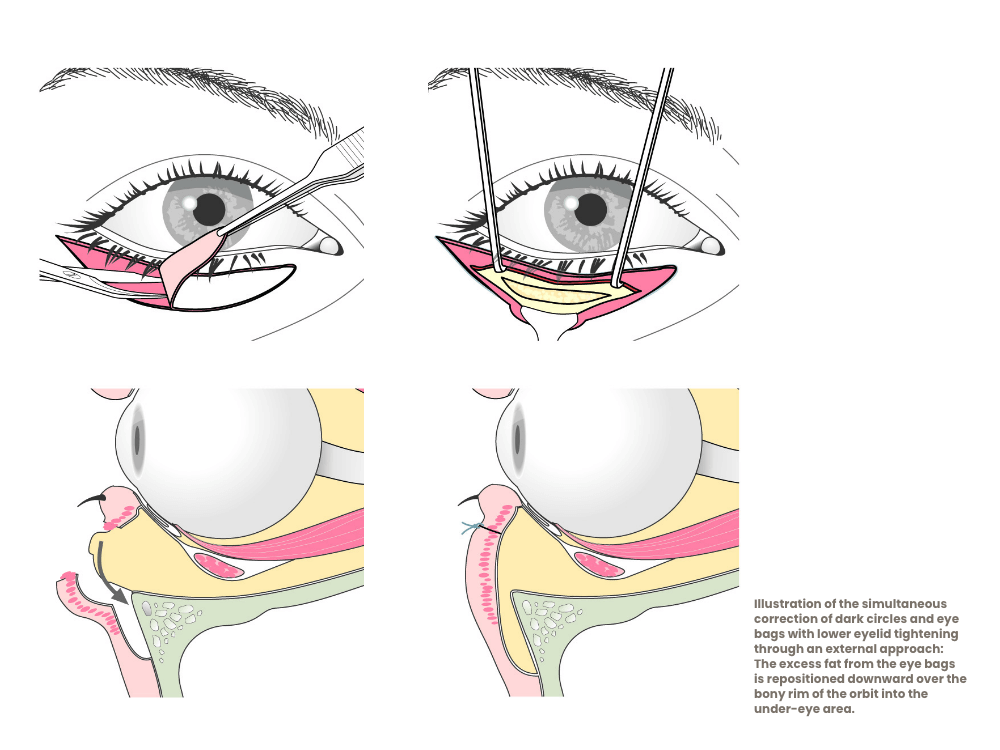
2) Eye bags combined with dark circles
In the past, the fat forming the eye bags was simply removed. However, when dark circles are present at the same time, this approach is not suitable for achieving an optimal aesthetic result in the lower eyelid area. The reason is simple: when both eye bags and dark circles exist, removing fat from the eye bags depletes the lower eyelid area, leaving the midface hollowed out — which is neither attractive nor youthful.
For about 25 years, I have therefore been performing combined correction of eye bags and dark circles as follows: the fat pads are mobilized and repositioned downward over the bony edge of the eye socket, thereby filling the dark circles. In principle, the excess volume of the eye bags is divided — half is used to fill the volume deficit of the dark circles. This procedure can also be performed through an incision on the inside of the lower eyelid if no simultaneous lower eyelid tightening is necessary or desired, making the operation scar-free.
In recent years, I have found a valuable addition to this procedure for my patients: just as with transconjunctival eye bag correction in younger individuals, it is often difficult to achieve a perfect result solely through fat repositioning. Sometimes the volume of the eye bags is insufficient to completely fill pronounced dark circles, or small irregularities remain between the repositioned fat pads. Therefore, I regularly combine this surgery with autologous fat transfer to fill any remaining unevenness or contour differences between the repositioned fat pads and the dark circle area.
Dark circles – with volume deficit
It is remarkable how many young patients come to me wishing to correct their sometimes very deep dark circles. Often, other practitioners treat this condition using hyaluronic acid (fillers) — in my practice, however, this is the exception. Fillers have the decisive disadvantage that the procedure must be repeated every 4–8 months. Therefore, although hyaluronic acid treatments can be effective in experienced hands, they ultimately become a real money pit and are considerably more expensive in the long run than autologous fat transplantation.
Correction of dark circles is simple and equally safe using autologous fat. Of course, this requires knowledge and experience — but that applies to any medical treatment. We always enrich the fat with PRP (platelet-rich plasma) to improve graft survival and to make the fat softer and more pliable, so that it can still be gently reshaped with the fingertip after the operation. If a single session is not sufficient (as the survival rate can vary), an additional fat injection is performed 10–12 weeks later. At that point, the desired correction or volume enhancement is almost always achieved. The procedure is performed under local anesthesia, using blunt cannulas with a diameter of 0.8 mm for fat injection. This method has always been well tolerated — both by women and by men, who, incidentally, tend to be more sensitive to pain than women.
There is usually sufficient autologous fat available. For this procedure, a small amount of fat is taken from the thighs or abdomen and transplanted into the lower or upper eyelid area. We always enrich the fat with PRP to make it supple and moldable and to improve its integration.
The procedure is very gentle and performed using a special injection technique. The results look completely natural, and there are no visible scars whatsoever.
Dark circles – pigmented, without volume deficit
Dark circles without a volume deficit can be lightened using a stem cell injection (nanofat).
Overview: Wrinkled lower eyelids, lower eyelid correction – how are sagging lower eyelids corrected?
Just like the upper eyelids or the facial skin, the skin of the lower eyelids can lose elasticity and become wrinkled due to the aging process. In principle, the correction of wrinkled lower eyelids is not technically very difficult: the skin is incised just below the eyelashes of the lower eyelid and carefully lifted from the underlying muscle. The excess skin is then assessed, removed, and the wound closed again.
Unfortunately, this operation carries a relatively high risk of a very unpleasant complication: ectropion.
If skin is removed from the lower eyelid area and even slightly more than the true excess is excised — or if the skin contracts more than usual during healing — or if excessive scar formation occurs in the subcutaneous tissue, then a downward pull is exerted on the lower eyelid margin. As a result, the lower eyelid turns outward and no longer rests against the eyeball. This extremely uncomfortable condition (complication) is called ectropion.
With every lower eyelid tightening procedure, it is essential to take great care to prevent this complication, as its correction is laborious, complex, and sometimes not fully successful.
Preventive measures / examinations to avoid ectropion
In principle, the elasticity of the lower eyelid can be tested using the snap test. The lower eyelid is gently pulled away from the eyeball, and the time it takes for the eyelid to return to its normal position is observed. If it quickly snaps back (hence the term “snap test”), the risk of ectropion is relatively low. If it takes longer than half a second to one second, special caution is required. In such cases, several additional measures must be considered during lower eyelid tightening to prevent the dreaded outward turning of the eyelid (ectropion).
These include:
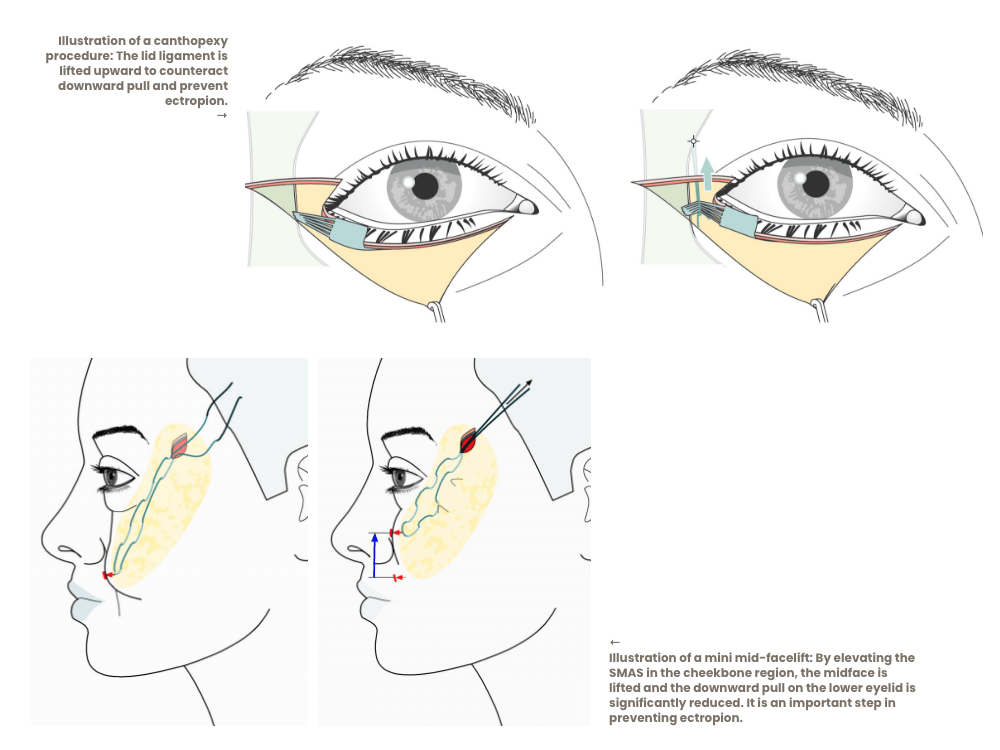
- Canthopexy
- Doubling of the SMAS layer beneath the lower eyelid
- Mini midface lift
- Muscle sling
All these techniques tighten the lower eyelid region or reduce the downward tension on the operated lower lid to prevent ectropion.
Canthopexy means slightly tightening the outer corner of the eye (unlike canthoplasty, where the eyelid position is deliberately changed — for example, to lift low outer eye corners in the case of a negative canthal tilt, see next section: correction of “hound eyes” → “cat eyes”). In this procedure, the outer edge of the lower eyelid is lifted and secured with a suture anchored to the inner side of the upper orbital rim (periosteum).
Doubling of the SMAS layer is performed by pulling the upper layer of the subcutaneous tissue (SMAS) upward and suturing it to itself near the outer corner of the eye, thereby reducing the downward tension on the lower eyelid.
The mini midface lift is a somewhat more complex but particularly effective procedure: at a suitable point in the cheekbone region, the SMAS is lifted upward with a suture and anchored near the chewing muscle (similar to the lateral brow lift). A pleasant side effect of this technique is that the nasolabial fold is also slightly reduced.
Muscle sling: The orbicularis oculi muscle surrounds the eye and is broad and strong. By lifting its lateral fibers upward, a kind of “hammock” is created that supports the lower eyelid and prevents it from sagging.
All these measures are technically demanding, quite time-consuming, and require significant experience to perform correctly and — most importantly — in the right degree. It is therefore not surprising that many physicians avoid or simply do not offer lower eyelid tightening to avoid being confronted with the complication of ectropion.
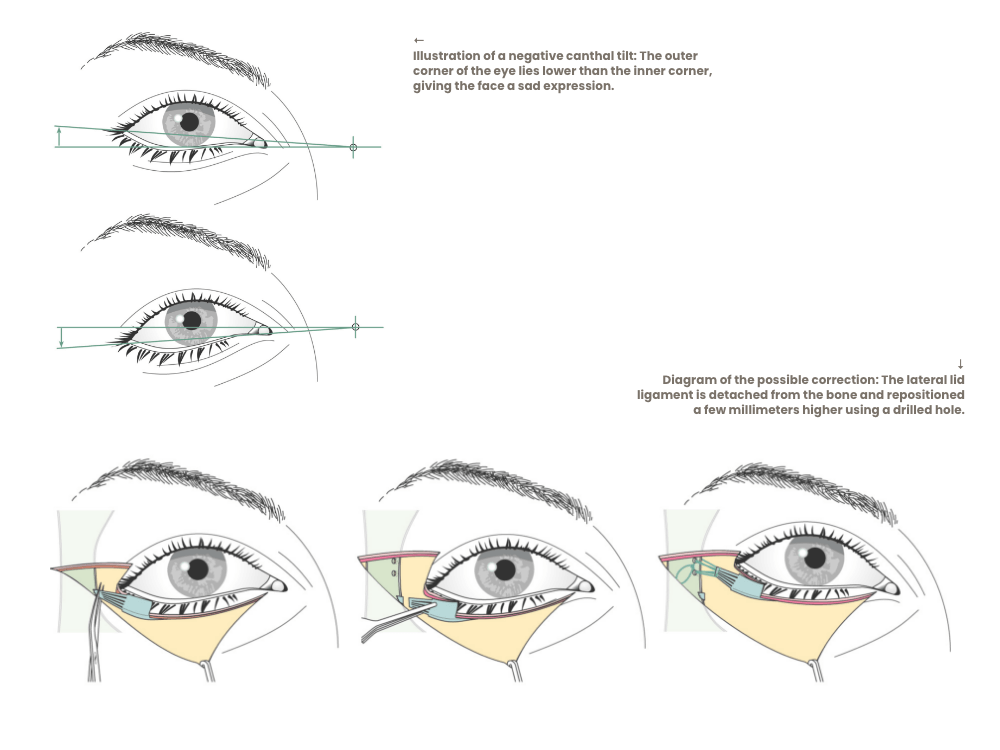
Canthal tilt
In some people, the outer corner of the eye lies lower than the inner one (negative canthal tilt). In Austria, this situation is often referred to as “hound eyes” (Dackelaugen or Dackelblick). This appearance can indeed be perceived as attractive (for example, Sylvester Stallone); some people like it, while others prefer higher outer eye corners because they favor almond-shaped eyes (“cat eyes”).
It is actually possible to lift the outer eye corner — this is done, among other methods, with a canthoplasty. During canthoplasty, the lower eyelid tendon is detached from the bone at the outer corner and then reattached higher up by drilling small holes in the lateral bony rim of the eye socket, allowing the tendon to be fixed in its new, elevated position. This procedure is technically demanding and requires extensive experience.
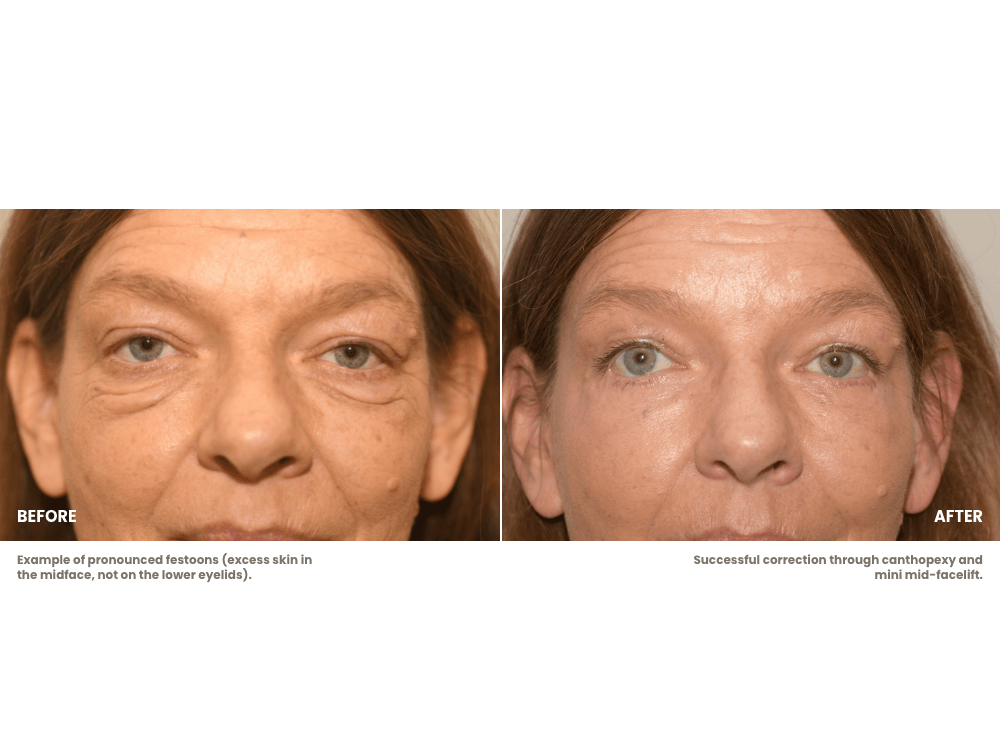
Festoons – anatomy and correction
Festoons are excess folds of skin in the midface area — that is, in a region well below the bony eye socket and around the cheekbone. Festoons can vary greatly in severity and are often perceived as very bothersome, even more so than sagging lower eyelids, because they are visible not only under the eyelashes but right in the middle of the face.
For patients seeking advice, it is often quite difficult to distinguish between wrinkled or sagging lower eyelids and festoons. Naturally, it is also possible for someone to have both excess skin on the lower eyelids and festoons at the same time.
When correcting festoons, it must be understood that this procedure extends well beyond the surgical field of the lower eyelid region. Essentially, the correction of festoons represents a type of midface lift. Consequently, much more skin must be lifted compared to a standard lower eyelid tightening. However, this does not necessarily mean that the incision has to be significantly longer: in most cases, even for festoon correction, the incision can be limited to the lower eyelid margin and extended just 1–1.5 cm laterally within a smile line, leaving virtually no visible scars after a successful procedure.
The correction of festoons must, of course, address the significant skin excess, but as already mentioned in the context of lower eyelid tightening, the risk of skin contraction/scar shrinkage is considerably higher in such an extensive procedure. Therefore, the correction of festoons can never consist merely of removing the excess skin. At the very least, a mini midface lift should be performed, or in extreme cases even a subperiosteal midface lift. Additional supportive measures such as SMAS doubling, canthopexy, and the muscle sling may also be necessary and beneficial.
In summary, the correction of festoons is significantly more complex and carries a higher risk than lower eyelid tightening alone. We have achieved good results in correcting festoons by combining several techniques: removal of excess skin, mini midface lift, SMAS doubling, canthopexy, muscle sling, and, if necessary, subperiosteal elevation of the midface.
Eyelid correction with laser
In the past, patients often asked me why I do not operate on eyelids (droopy eyelids) using a laser — since it was said to be modern, advanced, and scar-free.
Interestingly, I have not been asked this question at all in the last ten years, probably because the uselessness of this technique has become widely known. In fact, we plastic surgeons view this method very critically. When eyelid surgery is performed with a laser, the burning-hot laser beam is used as a scalpel — meaning the surgical principle is identical to that of a traditional scalpel. It is true that there is less bleeding, since the heat immediately seals (cauterizes) small blood vessels. However, it must be clearly stated that the use of a laser has no influence whatsoever on the surgical result. What else is done during surgery — for example, whether and how much fat is removed or added — is completely independent of laser use. The removal of skin (which is the only thing a laser can actually perform in aesthetic eyelid surgery) is of rather secondary importance.
Moreover, there are already publications recommending that laser incisions in the skin should be avoided, as they almost always lead to delayed or unsightly scar formation. For this reason, I do not use the laser, and it should be made clear that any claim suggesting an eyelid correction with a laser has any advantage is simply not true.